
Clinical Case: Is it possible to do more with less? Cracking the chameleon effect
Using 3M™ Filtek™ Easy Match Universal Restorative.


Molar incisor hypomineralization is prevalent worldwide, but there are no official treatment guidelines. This article presents a practice-approved concept.
We would like to learn more about your dental treatments offered in the pedriatic segment. Click here to complete a quick 5 minutes survey.
Molar incisor hypomineralization (MIH) is a qualitative developmental defect of the enamel, which can have a negative impact on general health and a patient’s quality of life. Treatment is usually demanding to both, the patient and the clinician. Affected teeth often develop advanced carious lesions, and they usually require immediate therapeutic measures as well as repeated restorative treatment. Based on years of experience in managing MIH, we have established a standardized three-step treatment approach:

Patient with several teeth including the maxillary severely affected by MIH.

lst view of the initial situation with exposed dentin on the affected first molars.

Situation after treatment of the demarcated enamel opacities in the anterior region with 3M™ Clinpro™ XT Varnish Durable Fluoride-Releasing Coating.

Final situation captured with a polarizing filter.

Occlusal view after covering of the exposed, hypersensitive dentin in the posterior region with glass ionomer restorative (3M™ Ketac™ Universal Glass Ionomer Restorative). The temporary coverage treatment was followed by a six-month remineralization period. Measures included toothbrushing with 3M™ Clinpro™ Tooth Creme and application of a product with CPP-ACP (GC Mi Paste plus) twice per day, and rinsing with fluoride mouth rinse after night toothbrushing.

Case 2: Moderate form of MIH
Initial situation of a patient with moderate MIH and post-eruptive enamel breakdown in the mesio-buccal aspect of the maxillary first molar. The areas affected by enamel breakdown were covered with glass ionomer restorative first, followed by a six-week remineralization period.

When the patient did no longer complain about pain or discomfort, the definitive restorative treatment was initiated. This image shows the isolated tooth after minimally-invasive preparation. It is beneficial to place the restoration margins in healthy enamel.

Etching of the prepared tooth structure and the surrounding surfaces with phosphoric etching gel.

Application of 3M™ Scotchbond™ Universal Adhesive to the etched surface. It is rubbed in for 20 seconds, air-dried for evaporation of the solvent until the layer appears solid, and light-cured for 10 seconds.

Placement of 3M™ Z100 MP Restorative. Using a brush, the restoration can be modeled and extended to cover the whole occlusal tooth surface.

In order to prevent the formation of an oxygen-inhibited layer, glycerin gel is applied and the composite cured though it.

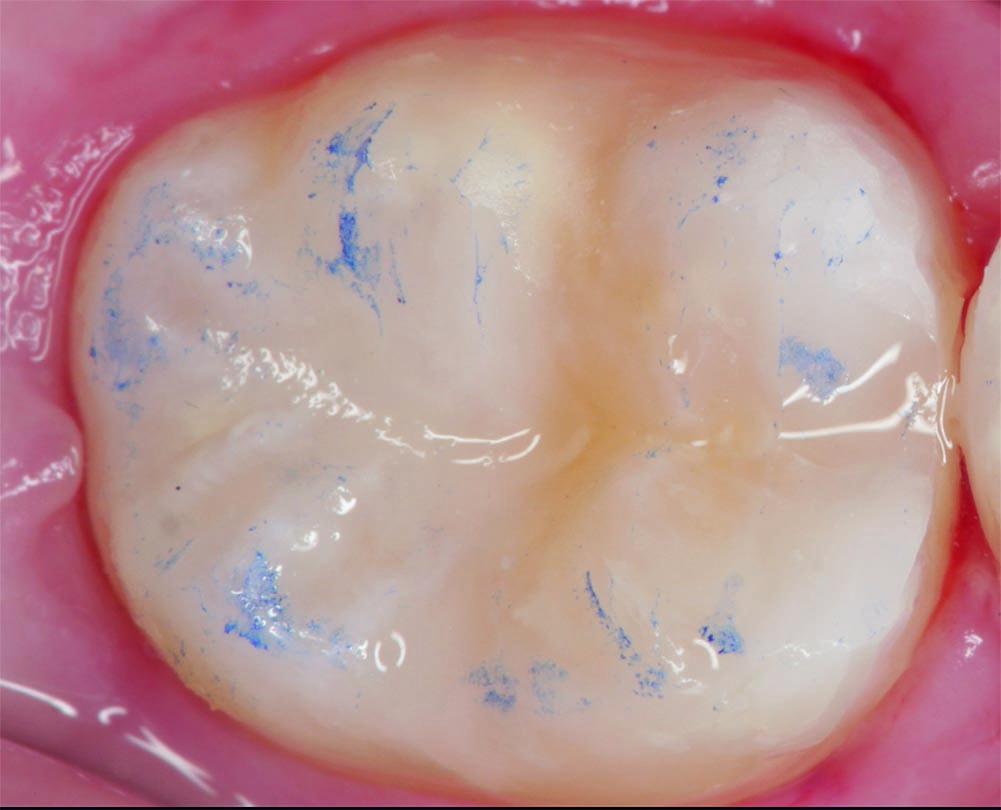
Treatment result after finishing, polishing and checking of the occlusal contacts.
Conclusion
Using the described concept, it is possible to treat most of our MIH patients successfully. According to our experience, the long-term stability of esthetic composite restorations is increased if we follow our remineralization protocol not only prior to restorative treatment, but also afterwards until the patient is fourteen to sixteen years old. Usually, there is no need to replace the restorations frequently (as otherwise typical for MIH patients). Sometimes, however, we need to repair them, which is possible without problems when using composite.
We would like to learn more about your dental treatments offered in the pedriatic segment. Click here to complete a quick 5 minutes survey.


Using 3M™ Filtek™ Easy Match Universal Restorative.

Using 3M™ Imprint™ 4 Light VPS Material, 3M™ Intra-oral Syringe, 3M™ Imprint™ 4 Heavy VPS Material, 3M™ Protemp™ 4 Temporization…

Using 3M™ Scotchbond™ Universal Etchant, 3M™ Scotchbond™ Universal Adhesive, 3M™ Elipar™ DeepCure-S LED Curing Light, 3M™ Filtek™ One Bulk Fill…