
Who wrote the reference book “Le chirurgien dentiste” from 1728?
Brain of the Week – History


In dentistry, the term adhesion is often used to refer to mechanical bonds that can be achieved by means of micro-retentions, with or without chemical interaction between the substrates. This is the bond between the etched enamel and the fluid composite containing the dentin adhesive system1.
Since the direct bonding of orthodontic appliances was first described in 19652, Solventum (previously 3M Health Care) has introduced products designed to improve treatment mechanics and simplify orthodontic procedures. After almost 70 years of evolution in orthodontic adhesive bonding, today we routinely bond orthodontic appliances with composite resin-based adhesive systems, a pivotal technology that has contributed most to efficiency in orthodontics.
The most recent adhesive systems include selfetching solutions. They arise from the need to reduce the number of clinical steps and decrease the probability of error in manipulation. These are based on the use of monomers that include acidic groups attached to the primer components. The function of the acid monomers is to exert the action of the acid etch and the primer, producing demineralization of the dental tissues while wetting the substrate and preparing the tissues for the subsequent infiltration of the composite monomers. This is particularly critical in restorative dentistry when generating each hybrid on dentin.
Self-etching agents offer some advantages over conventional acid etching techniques: a more homogeneous etching pattern, faster application and reduced risk of contamination3.
There are currently no self-etching agents that exceed the bond strength achieved by etching the enamel with orthophosphoric acid. However, the resistances observed with self-etching agents are sufficient, reducing the damage to the enamel, especially when the appliances are removed. When comparing in vitro acid etching with self-etching agents, it has been found that Transbond Plus Self Etching Primer is the only one that does not significantly affect the resistance to debonding of brackets4.
![]()
![]()
![]()
![]()
Attachments are important to achieving treatment outcomes in aligner therapy. They are used to improve retention, allowing the aligner to exert more precise and effective pressure on the tooth.
Their differences in size and position make the preparation of the tooth with conventional acid etching sometimes uncomfortable. In order not to etch more than necessary, we must constantly check the stencil where the acid is to be applied, which is time consuming. Many times we end up over-etching the surface, unnecessarily affecting enamel that has nothing to do with the bonding of these small attachments.
For these purposes, the use of Transbond Plus Self Etching Primer in the bonding of attachments is particularly convenient and practical. It is a self-etching agent that uses a paddle system containing three compartments; by pressing the first one, the contents drain into compartment two and then both components pass into the third compartment, where the mixture is finished with an applicator.
As a self-etching primer, it is less aggressive than a conventional acid etch. It can be applied precisely on the intended surface of the tooth without significantly affecting the surrounding enamel that will not be in contact with the attachment.
![]()
This new solution from Solventum is a hybrid composite of fluid consistency, composed of bisGMA, TEGDMA and Procrylate composites activated by visible light. The product is stored in multi-purpose syringes to be used with single-use dosing tips.
Its filler is a combination of ytterbium trifluoride with a particle size range of 0.1 to 5.0 microns, a 20 nm surface-modified non-agglomerated/non-aggregate silica filler, a 75 nm surface-modified non-agglomerated/nonaggregate silica filler and an aggregate zirconia/surfacemodified silica filler (consisting of 20 nm silica and 4 to 11 nm zirconia particles).
The aggregate has an average clumping particle size of 0.6 to 10 microns. The inorganic filler loading is approximately 65% by weight and 46% by volume.
One of its most important characteristics is its thixotropic fluidity, decreasing its viscosity during the application of pressure. The syringe has been designed to minimize the generation of bubbles that could compromise the shape and adhesion of the attachment. The disposable tip is small allowing precise filling of the wells in the
attachment template and once the process is completed the composite returns to its original viscosity without dripping.
By bringing the template into the mouth and applying pressure this property again allows the composite to adapt to the morphology of the tooth and distribute evenly. This not only facilitates the placement of the attachment, but also aids in its integration with the tooth enamel.
If too much composite is applied, it can be easily removed with a bur, scaler or periodontal curette. Conversely, incomplete filling of the attachment template may result in a gap compromising the shape and adhesion of the attachment. However, in my clinical experience, I have found the composite is easy to work with.
Aesthetics is another crucial factor in the choice of the composite to be used in attachment creation. Clarity Attachment Material is available in only one shade, but has translucent properties that allow good blending with different shades of teeth. It requires virtually no polishing and its enamel-like fluorescence makes it a good choice.
![]()

It is crucial to start by cleaning the tooth, removing all plaque and debris. Remember that we will not perform a conventional acid etching, which has the ability to remove some of the organic matter. Perform a dental prophylaxis with water, pumice or oil-free paste and then rinse. Isolate the teeth using lip retractors, dry-angles or cotton rolls, dry using a source of air without oil or moisture.
Test the attachment template to ensure that there are no fit problems attributable to template fabrication or unnoticed post-scan restorations.
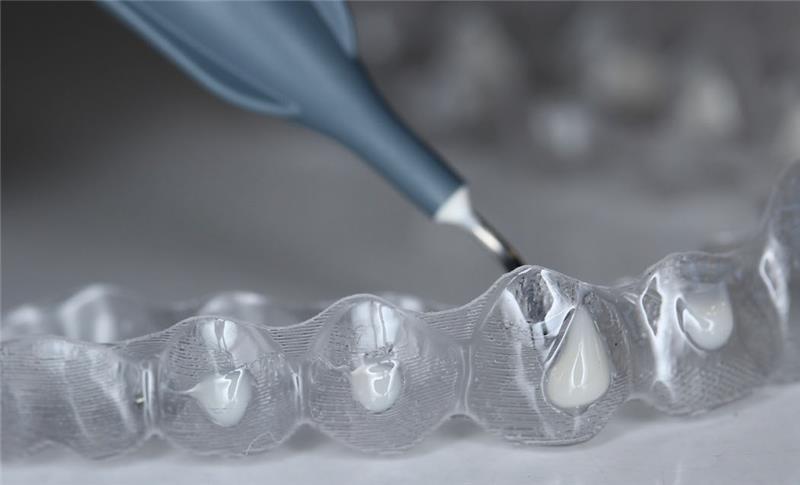
Remove the cap from the syringe and attach a new applicator tip. Bring the tip to the deepest part of the space to form the attachment and without lifting it, begin to press until the composite begins to drip out. Fill completely paying special attention to the angles and surfaces that will be in contact with the tooth.


The amount of primer on a pallet has been calculated to cement brackets and tubes in a complete arch. In my experience it is usually sufficient to cement attachments of both arches in one patient. Once the teeth have been prepared, proceed immediately with bonding. Do not use the applicator on more than one patient, the primer mixed in compartment 3 will lose its properties when stored.

Take the pre-filled template into the patient’s mouth. Press it with your fingers or with the help of a scaler so that it adapts closely to the contour of the tooth and the excess composite can flow as a small film around the attachment. During this step, make sure that the cuvette is well positioned in the patient’s mouth. Correct positioning is key to ensuring that the composite flows to the correct area and stays in place during the polymerization process.
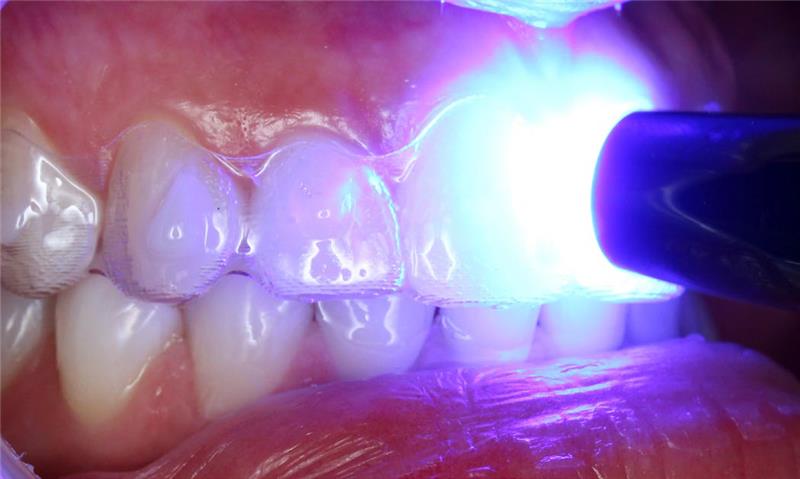
Hold the stencil in place and polymerize each attachment for a minimum of 6 seconds with a 3M™ Ortholux™ Luminous Curing Light. The curing light should be directly over the fixation site, perpendicular to the fixation site and as close as possible to the template. If using another manufacturer’s curing light, refer to the manufacturer’s Instructions for Use for proper light curing technique. Once the curing process is completed, remove the template with the aid of a scaler by first removing it from the lingual area of the molars.

Once the template has been removed, confirm the correct union of each of the attachments, absence of gaps between the composite and the tooth. Clean off any excess with a bur or scaler. In case of adhesion failure or if a gap between the tooth and the attachment is detected, remove the composite from the surface with a bur and repeat the process.

A minimal final polishing with prophylactic paste is recommended to leave the surface of the attachment smooth and free of irregularities, contributing to better esthetics and greater comfort for the patient.
The use of Transbond Plus Self Etching Primer is an aid when making attachments in orthodontics with clear aligners. Fewer steps involve fewer operator-attributable errors. The work is faster and more comfortable since we do not have to be as concerned about over-etching unnecessary areas as with the conventional etching method, nor does it require the rinsing stage. Special attention must be paid to the thorough removal of organic matter that may exist on the tooth surface and the elimination of excess primer to ensure good adhesion of the attachments.
The Clarity Attachment Material properties, together with the design of its syringe, allow simple handling, reducing the formation of bubbles, easy removal of excess, minimum need for polishing and a good mimetic capacity with the dental enamel. I have found it to be an excellent choice when choosing a composite for making attachments.
We would love to know how we can improve the blog for you. Please answer our survey below. It only takes a few minutes.
You can answer anonymously if you prefer.
Authored by: Roberto Vogel Alvarez, Dental Surgeon, Specialist in Orthodontics, Academic Postgraduate, Orthodontics University of the Frontera Temuco, Chile
1. Hatrick C. D., Eakle W. S., Bird W. F. (2012), Dental materials. Clinical applications. 2nd ed. Mexico: Editorial El Manual Maderno
2. Newman, G. V. (1965), “Epoxy adhesives for orthodontic attachments: progress report”. Am. J. Orthodontics and Dentofacial Orthopedic, 51 (12): 901-12
3. Scougall Vilchis R. J. (2010), “Scientific evidence for the application of self-etching agents in clinical orthodontics”. ADM Journal, LXVII (1): 8-12.
4. 20. Scougall-Vilchis RJ, Ohashi S, Yamamoto K. Effects of 6 different self-etching primers on shear bond strength of orthodontic brackets. Am J Orthod Dentofacial Orthop 2009; 135: 424.e1-e7.
Brain of the Week – History
Brain of the Week – Chemistry
Brain of the Week – Fun Facts